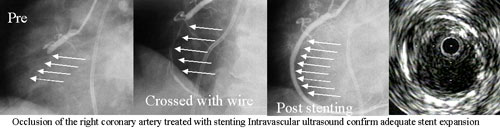
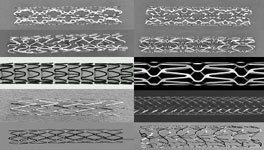
Stenting has revolutionized Interventional Cardiology resulting in higher (99%) acute success rate and lower rates of restenosis (renarrowing). Interventional Cardiologists at BIDMC helped develop and studies these procedures and pioneered the use of stents (implanting the first stent in coronary arteries in 1988). Stents come in different designs and configurations including slotted tubes, coils, meshs, ….. Stents are delivered while collapsed and are then deployed using a delivery balloon and may be postdilated to achieve a perfect result. Stents remains in the artery permanently, holding it open, and preventing restenosis (and remodeling). Stents are used in 70-80% of interventional procedures due to their reliability and predictable results and their beneficial effects on restenosis. Reclosure (restenosis) is also a problem with stenting procedure, but at a rate lower than baloon angioplasty alone. Drug eluting stents or medicated stents have reduced risk of restenosis and are overwhelmingly used in revascularization. A problem unique to stents is acute of subacute thrombosis of the artery after successful stenting. However, this risk is reduced to <1% by antiplatelet agents (Aspirin and Plavix) and good stenting technique. Adequate stent deployment and expansion (often confirmed vy intravascular Ultrasound) achieving near perfect acute results are crucial to reducing the risk of thrombosis and the delayed risk of restenosis.